What are possible interventions?
Building blocks of the treatment
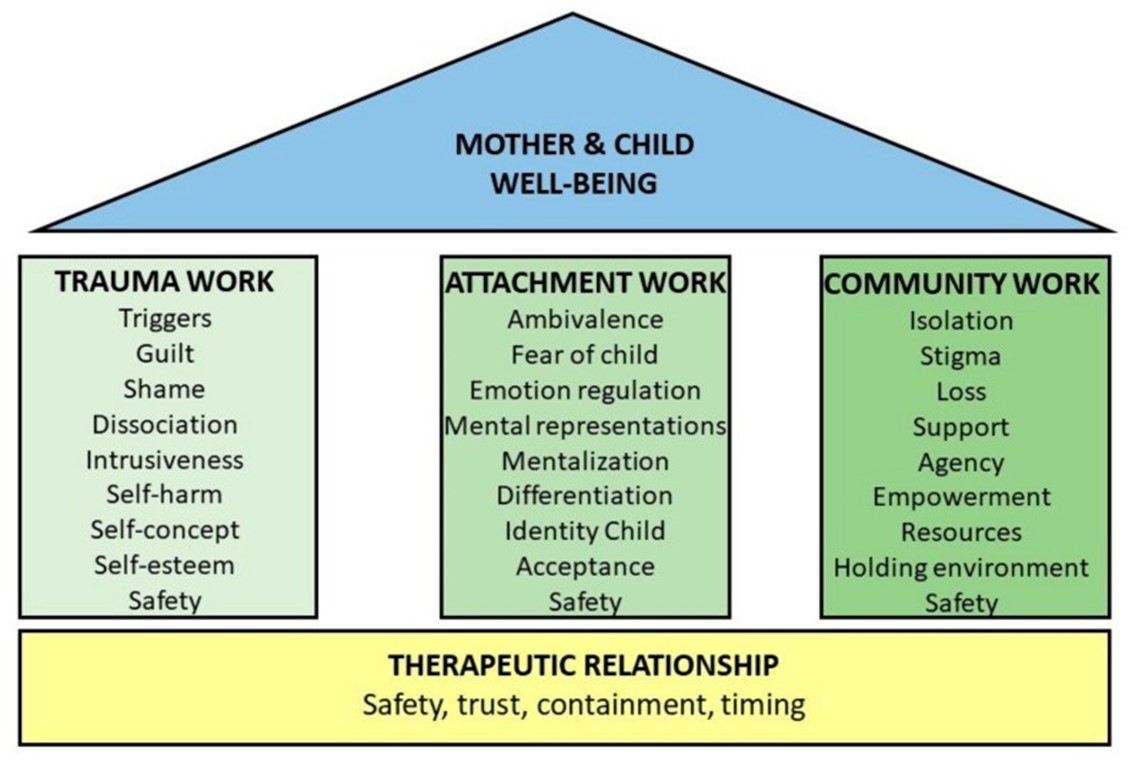
Research has identified the global expertise of professionals in treating mothers with a child born of sexual violence (1, 2). This showed that there are three building blocks that together contribute to the well-being of mother and child. These building blocks are the following:
- assistance in reducing the mother's trauma;
- improving the attachment relationship between mother and child;
- improving the position of mother and child within the community.
Professionals believe that by combining these three building blocks, they can provide effective treatment to mothers with a child born of sexual violence, and to the child itself. Focusing on one building block, for example trauma treatment or the parent-child relationship, is considered ineffective. The three building blocks each contain interventions that may be used by professionals. It is notable that every building block contains the theme of safety. A continuous focus of attention in the treatment is the safety of both mother and child, both inside and outside the treatment room.
For the attachment relationship building block, it appears that interventions consisting of psychotherapy, psychoeducation and skill training are most effective in promoting the well-being of traumatised mothers and children (3,4). For this reason, it is good to offer a combination of interventions. Interventions are based on the assumption that a mother must meet her own needs in order to meet the child's needs. This is why psychoeducation and skill training focus on building blocks one and three, for example promoting social support, developing coping skills and making time for relaxation.
Relationship of trust
As can be seen in the figure below, the relationship of trust between professional and mother plays a major role. The effectiveness of interventions seems to be determined by the ability of a professional to establish a safe therapeutic relationship with the mother and the child (1). In this therapeutic relationship, meaning is partly created "because you gradually get closer until you stumble onto something that is understood both by the therapist and by the client" (2). This means: taking the time to reflect together on what are important experiences for the mother. This leads to a shared understanding. In this difficult-to-reach population with complex needs, a safe therapeutic relationship not only contributes to the effectiveness of interventions, but is also the cornerstone that makes interventions possible.
A therapeutic relationship can be shaped by focusing on the following points:
Trust and safety
Trust and safety are essential in the relationship. For example, the mother knows that you are available and reliable. Therefore, be aware of your own assumptions regarding sexual violence, motherhood and assistance.
Understanding
Invest sufficiently in the mother within her specific context. The problems of these mothers are layered and only by a good understanding of them will you be able to find the right interventions for this mother and this child.
Connecting at the mother's pace
Take sufficient time to listen to the mother and help her and allow her space to talk, and to stay silent. Not all questions need to be asked immediately, not all answers need to be given immediately.
Treatment methods
1) Focused on reducing trauma-related complaints
The guideline for PTSD recommends Cognitive Behavioural Therapy (CBT) including Imaginary Exposure (IE) and Eye Movement Desensitisation and Reprocessing (EMDR) (5). The preferred treatment for refugees is Narrative Exposure Therapy (NET). It is important to understand that the mother-child relationship is part of the trauma treatment, because the mother may be triggered in this relationship. It is therefore important to combine interventions aimed at processing trauma with interventions aimed at the attachment relationship.
2) Focused on the attachment relationship between mother and child
There are no specific relationship-focused treatment methods for this group of mothers with children. Given the complexity of the problem, it will often not be sufficient to only carry out the standard treatment protocol. More often, the protocol will need to be adapted to the specific context of this mother and child.
The NJI provides a good overview of available evidence-based and best-practice treatments.
Elaborating interventions in the event of attachment problems| NJI
Examples of interventions aimed at optimising the parent-child relationship are: VIPP, NIKA, Video Home Training, Child-Parent Psychotherapy and Parent-Child Interaction Therapy.
In the case of young mothers or mothers who raise their children outside their own community, it is often desirable to combine interventions aimed at sensitive parenting with interventions aimed at parenting competencies.
Low-threshold interventions are important because the threshold for care for this target group can be high. On the one hand, mother and child can be supported at an early stage, on the other hand, they pave the way for follow-up support for those who need them. Low-threshold interventions can include: a mother and baby group (this is available in many locations) and preventive home visits by, for example, Precautionary Care of the GGD.
Precautionary Care is a proven effective programme that is being given in an increasing number of places in the Netherlands.
Check the website for precautionary care
3) Focused on the position of mother and child in the community
The development of interventions aimed at breaking down stigmatisation are limited within the framework of aid. However, this does not mean that we are empty-handed when it comes to working with this target group. During treatment, focus on developing a social support system around mother and child. This will help them function in their daily life, and in breaking stigma. Talk to the mother about her perception of her position in the community and what she wants to do in this regard. Experience shows that the way in which mothers find their way in this is very individual. The therapist can explore and support the various choices with the mother. Finally, be aware of your own views about sexual violence and motherhood that may contribute to stigmatisation. Use peer review to reflect on your own process.
(Check out the page Together we know more!?)
Check this video for more information about treatment of patients with trauma: